Lighting in hospitals and other healthcare settings is in transition. Each space within the building is being recognized for its different occupants’ needs. Strategic deployment of digital lighting in terms of lumens, color temperature, placement and personal control is now being given far more consideration. It’s a nesting doll of lighting—one space and one scenario followed by another.
“The hospital is not a single thing anymore,” said Randy Guillot of Gensler, a global design and architecture firm with 48 locations worldwide. Guillot, based in Chicago, serves as principal architect and design director for the firm and is also co-global health and wellness practice leader.
“There are many different healthcare spaces. We see a lot of specialty clinics and outpatient work. There is an enormous future in nursing homes or assisted living, too. Design principles for a healthy healthcare space as it applies to hospitals carries over to these other facility types. Lighting plays a huge part. Health and wellness are the largest growth area for Gensler,” he said.
Hospital owners and administrators are switching to LED lighting, and it is driven by saving energy and lowering costs including maintenance, which is a secondary consideration that has taken hold.
“Energy savings may have driven LED adoption in the healthcare sector, but, from a design perspective, that’s just the beginning,” Guillot said. “We are at a place with lighting where there is an opportunity to take a human-centric design perspective, a design to best benefit the people occupying a hospital from the patients to the staff. That’s a shift.”
The shift

Chad Beebe serves as deputy executive director for advocacy for the American Society for Health Care Engineering (ASHE), a subsidiary of the American Hospital Association based in Chicago and Washington, D.C. ASHE advocates for healthcare facilities including code compliance and development as well as tracking emerging trends and technologies. Lighting is covered in its “Guidelines for Design and Construction for Hospitals and Outpatient Facilities” including lighting levels based on the space. ASHE’s input helped guide NFPA 70 (lighting), and NFPA 99 (healthcare facility codes).
“A lot of our work deals with the impacts of lighting on patient care and benefits of good lighting for staff, as well,” Beebe said.
“When LEDs became a solution for better lighting life and cost, hospitals moved ahead with a ‘let’s do it and be done’ mindset,” Beebe said. “But then color rendition was off. If all your patients are blue, that was a problem. LED adoption has been a matter of discoveries. Brightness levels and color have since been major discussion points over the last 10 years. Because lighting is a big consumer of power for hospitals, LEDs are very attractive. The better we understand them, the more advantages they offer.”
Kathryn Caspar is vice president of indoor products for Cree Lighting, part of Ideal Industries Inc., based in Sycamore, Ill. “A clue to new lighting attitudes can be found in how new modern-day healthcare facilities look. These facilities are more attuned to patient comfort demonstrated through wall color choices [and] distinctive artwork. Work settings are getting more comfortable, too. Not addressing lighting would represent such a blind spot for a market now focused on the health and well-being of patient and staff,” she said.
Caspar sees much more consideration given to design when it comes to today’s LED luminaires.
“The sun’s shift during the day and your circadian rhythm is a big focus,” Caspar said. “That wasn’t a discussion 20 years ago. Now we are looking at artificial light that can mimic daylight as it rises and falls be it through tunable light or full-on circadian lighting systems. Some studies estimate we spend as much as 90% of our day indoors under electric light. The importance is starting to sink in as we look at our bodies as originally designed not receiving the right amount of light when indoors, and blue spectrum light shifting to red around 3 p.m.”
Caspar said encouraging research is finding that controlling LEDs to mimic natural light can positively affect the human body from healing to mood. Such information is providing a second wave of salesmanship as it educates clients, designers, manufacturers and contractors. Finding that research is not as hard as one might think.
ASHE’s Beebe recommends searching the Center for Health Design’s website (www.healthdesign.org/knowledge-repository) for lighting-focused research projects.
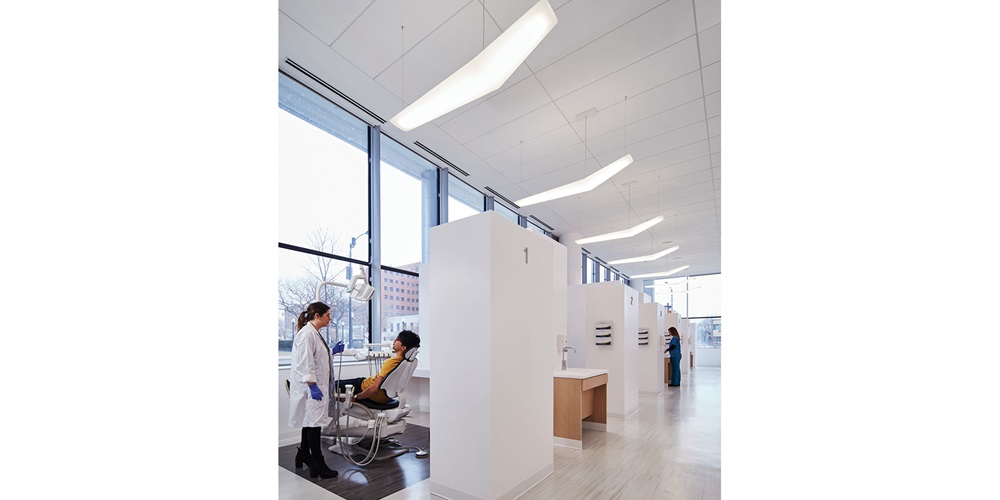
Differing spaces

Lighting in a hospital is far from one size fits all, but it wasn’t always that way. The same fluorescent lighting used at a nurse’s station illuminated a hallway, the emergency room and a patient’s room. The variety of spaces hasn’t changed, but rethinking the lighting needs for each is quickly moving front and center. There are many opportunities, but they can be complex. Think of a myriad of different labs, special care units, maternity wards, patient receptions, waiting areas and cafeterias. The knowledge and capability to light them insightfully plays into a market where buyer consolidation goes hand in hand with modernizing the hospital and other healthcare properties. In general, there seems to be a dual focus in lighting design. One is to provide comfort and calm for patients. The other is to keep staff sharp and focused.
“In a patient room, we want full lighting control, which would include more natural light,” Beebe said. “Maybe you also take functions out of the patient’s room such as reading charts to avoid the jarring evening disruption when a doctor or nurse flips a switch, flooding the room with LED light. Maybe you incorporate task lighting, which is something ASHE also provides guidelines in regards to usage and lighting levels. A shared room poses its own lighting control challenges, but most hospitals are moving to private rooms.”
Beebe added issues of LED color temperature and comfort are making their way into staff areas, which creates different strategies.
“You want to be consistent with your lighting types. You don’t want an LED-lit nursing station and fluorescent hallways. The work areas for nursing staff is different because it features egress lights and 24/7 lighting. You may want to save energy, but occupancy sensors but may not be the right approach and certainly not in patient rooms.
“Maybe a step-dimming approach could work. Circadian-rhythm systems could provide value in supplying the right light for staff,” he said. “For instance, night shift workers sleep during the day and need that daylight quality at night when they work. Circadian systems could play a role. Those same systems in neonatal care units may not be suitable for premature babies because they do not have a fully developed circadian rhythm. So, we steer clear of natural light or something that might simulate it.”
An operating theater has its own needs.
“Early LEDs used for surgical light cast an unnatural surface light,” Beebe said. “Color is important to the surgeon, so they see what are operating on in a natural color. LED tuning is important. Something that was unanticipated with LED light was its cool operation. Surgeons were taking advantage of the heat cast from nondigital lighting sources. The challenge with LED was how to rebalance the room’s HVAC.”
The use of demos

While other markets may occasionally incorporate demo spaces to try out lighting strategies, this practice is readily adopted in healthcare.
“Coordinating with our customers so we are on the same page is so important,” said Jill Mahaney, senior associate-interior design at Gensler. “We find the use of demo spaces or mock rooms so useful when designing spaces for today’s healthcare. Having a mock exam or surgical room gives us the ability to test out design ideas and fine-tune. Lighting and lighting control choices are something we want to test. With monitors, cameras and other equipment, lighting plays a role in how they are read [e.g., glare] or capture images. Lighting’s interaction and its variables can be encountered in the mock-up and modified, if necessary, before the final design.”
Guillot said the mock-up also provides an opportunity for direct observation and feedback from the client, consultants, contractors and others. There is also the convenience of the demo often located on-site at the hospital.
“In a hospital space, adding new lighting is more than just fitting out the fixture,” Caspar said. “In a hospital room, there are several pieces of equipment to contend with, including oxygen and a different type of HVAC system that incorporates disinfectant. There are more data lines, as well. The plenum space gets very complicated. There are also requirements beyond pulling a permit. You are dealing with critical care. I think mock-ups are critical.”
The engaged electrical contractor
Electrical contractors that have traditionally served the healthcare market may have a leg up in winning work, but other ECs can gain favor.
“I was an architect” Beebe said. “In fact, I used to have a design-build company. I always valued an EC who was open to considering new technology, aware of what was out there and able to identify the needs of individual spaces. I appreciated the EC that had the ability to readjust as the project dictated, have the bandwidth to go beyond a ‘rinse and repeat’ approach to the work and recognize something new might be considered.”
“Everyone needs to better understand the demand of lighting in today’s healthcare setting so we can all get it right. It’s education all around,” Caspar said.
About The Author

GAVIN, Gavo Communications, is a LEED Green Associate providing marketing services for the energy, construction and urban planning industries. He can be reached at [email protected].